Neuro-biologist JJ Couey, reviews Nick Hudson’s Oct 11th presentation to the Actuarial Society of South Africa. A plain version can be watched on Pandata.org
(Apologies for the text/chat replay on the screen. Nothing I can do about it.)
Transcript
Copied from the Pandata substack. Contains an Addendum responding to some questions he was asked on the day…
Most of us are old enough to remember how bad models were so implicated in the 2008 financial crisis. The dawn of the Covid phenomenon was greeted by a plethora of models predicting doom of strikingly similar scale and, without exception, utterly failing to describe reality even vaguely. Those models generally assumed that there was a deadly virus and that lockdowns would “slow the spread” of it, resulting in less dying. One would call the results comical if their impact on society hadn’t been so tragic.
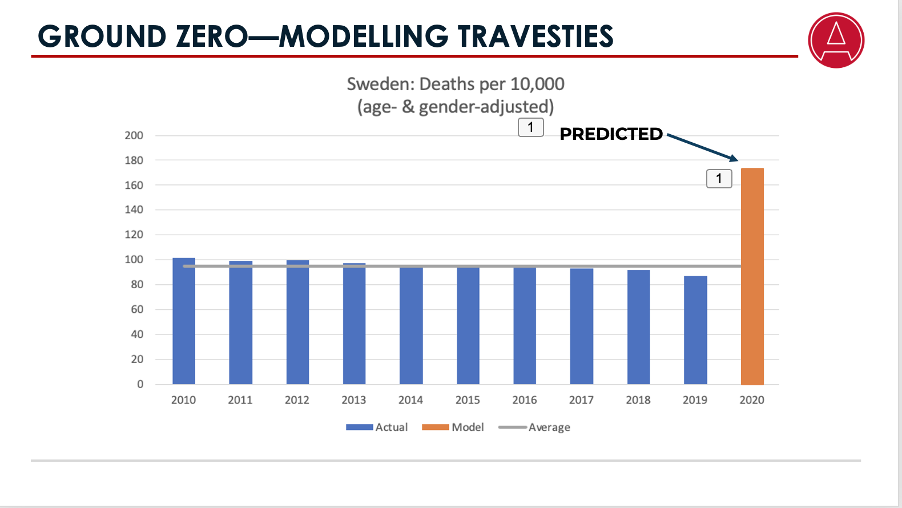
When Sweden famously rejected the lockdown construct, the modelers who facilitated the locking down of the world projected that it would experience, in a few short weeks, a whole year’s worth of death, translating into a weekly mortality rate some six times normal levels. That would leave them, at the end of the year with twice the level of normal deaths. What actually emerged was that Sweden had a year of mortality in line with its ten-year average.
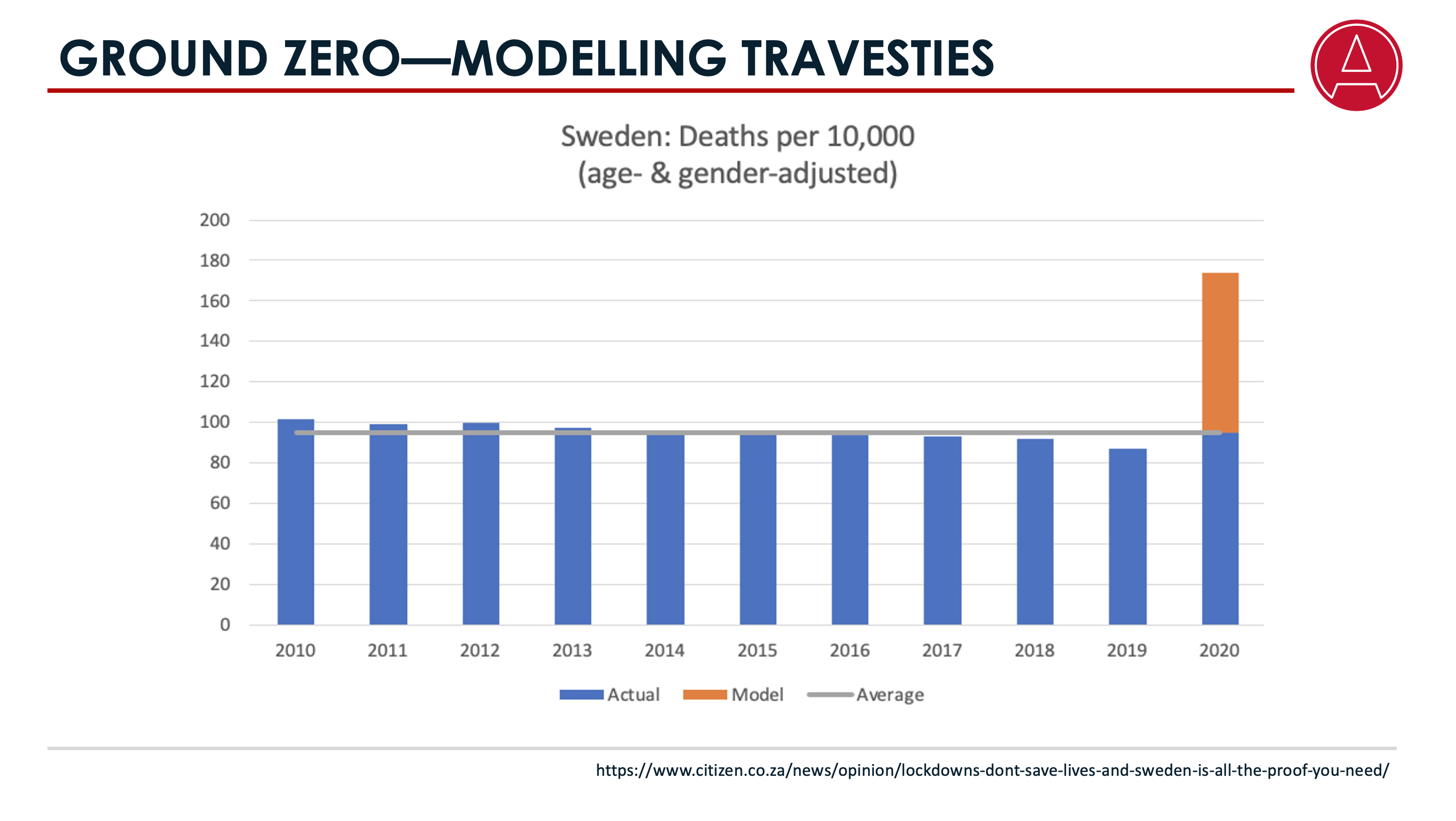
In our actuarial studies we learn about a little thing called the actuarial control cycle, which amongst others entails testing our models against emergent evidence. In commercial settings, failing to employ the control cycle after a signal as loud as this one would likely result in the responsible actuary facing some very difficult questions.
Now, the evidence that those models—called SIR models, standing for Susceptible-Infected-Recovered models—were not merely incorrectly calibrated, but wholly inappropriate for application to the Covid phenomenon, AND that the ensuing policy recommendation was wrong, was available abundantly, and available decisively, within weeks of the onset of the hysteria. But it was ignored. It was as if the control cycle had never been invented.
At PANDA, the organization I co-founded along with a group of multidisciplinary professionals to push back against the catastrophic hysteria, we could see, for example, …
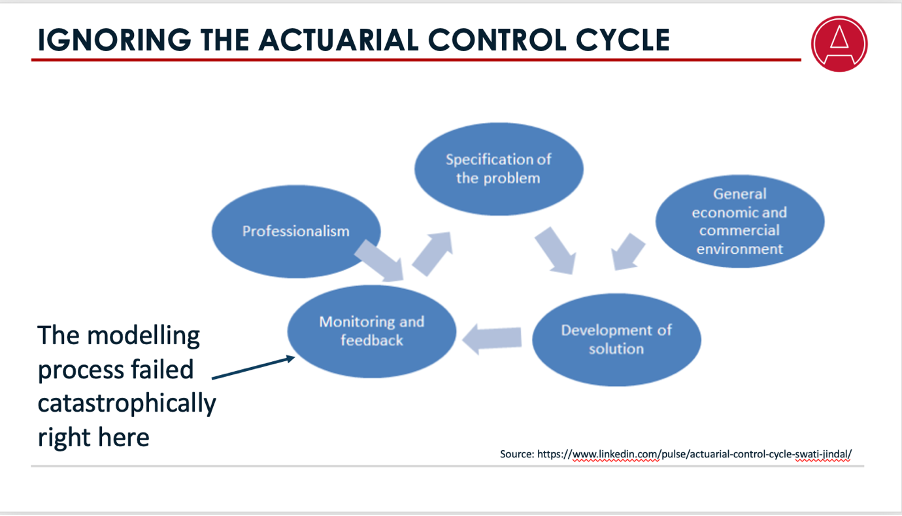
… that different places with similar population characteristics experienced completely different mortality outcomes, and that these differences could not be explained by viral dynamics. Something else was at work. This observation led us to adopt an empirical modelling approach capable of subsuming all factors, not just the theory of a novel deadly virus.
And, despite not being perfect, that model was very accurate. As the South African Coronavirus Modeling Consortium and the Actuarial Society continued to deploy SIR models, we outed their inaccuracy by making various predictions that were strongly validated by emergent evidence.
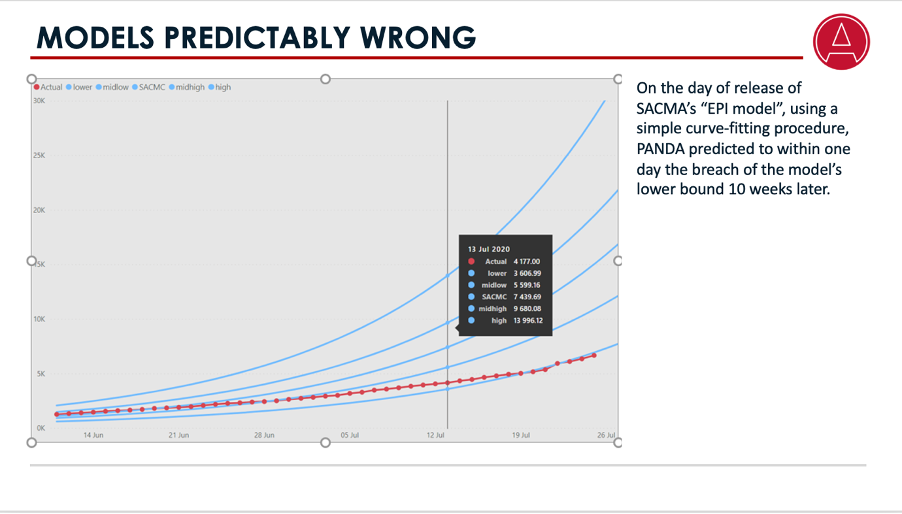
For example, at the time of release of SACMA’s revised model, we predicted that it would breach the lower bound of its comically broad confidence intervals in ten weeks. We were out by one day. Similarly we predicted that hospital bed demand would be just 5% of what they projected, again correctly. In the Western Cape, our model predicted peak utilization to the digit.
In December of 2020, we engaged with the Premier of the Western Cape. We asked him what had made him spend hundreds of millions building two field hospitals. He said that was what the models told them they would need. We described the inaccuracy of the SACMA models to him and he said he wasn’t using them—that he was using the ASSA model. He then astonished us by saying he was investing in a third facility, which like the other two, was eventually to close unutilized. As it turns out, it seems it was not ASSA who was advising him, but a consulting firm, using one of the varied but consistently wrong scenarios from the second iteration of the ASSA model.
I hope that his claim will be investigated and the failure by whatever actuarial consulting firm this was to comply with normal actuarial control cycle procedures will have consequences, because the public interest was certainly not protected.
But building pointless facilities was the least of the travesties unleashed against the public by woefully advised and highly pressurized governments. The financial and humanitarian consequences of lockdowns have been staggering.
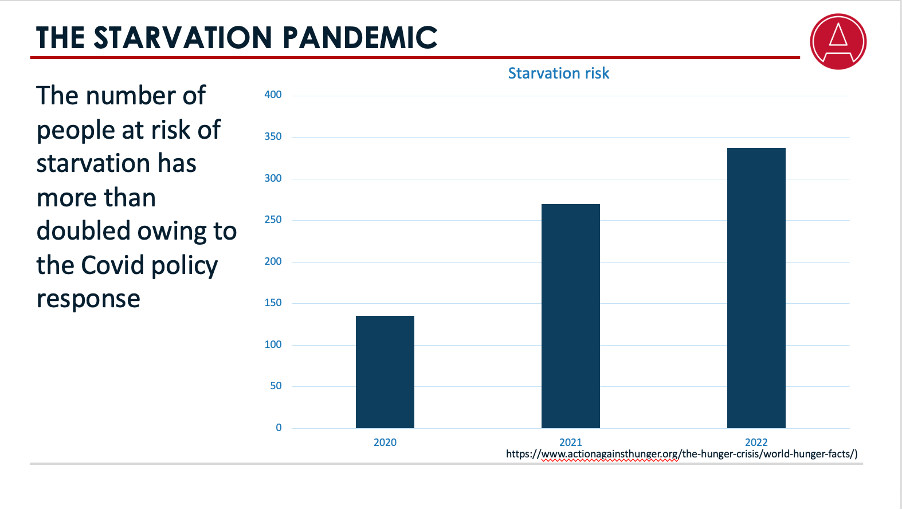
The established NGO Action Against Hunger finds as follows: Before COVID lockdowns, the number of people at risk of starvation was 135 million worldwide. By the end of 2021, that had increased by another 135 million people, and in 2022, it then increased by a further 67 million. The result is that we currently experience about 10 million new deaths per annum from starvation, 3 million of them among children.
On top of that, about 4 trillion dollars of wealth has been siphoned off from the middle classes to the benefit of a coterie of billionaires, the number of whom swelled by a quarter.
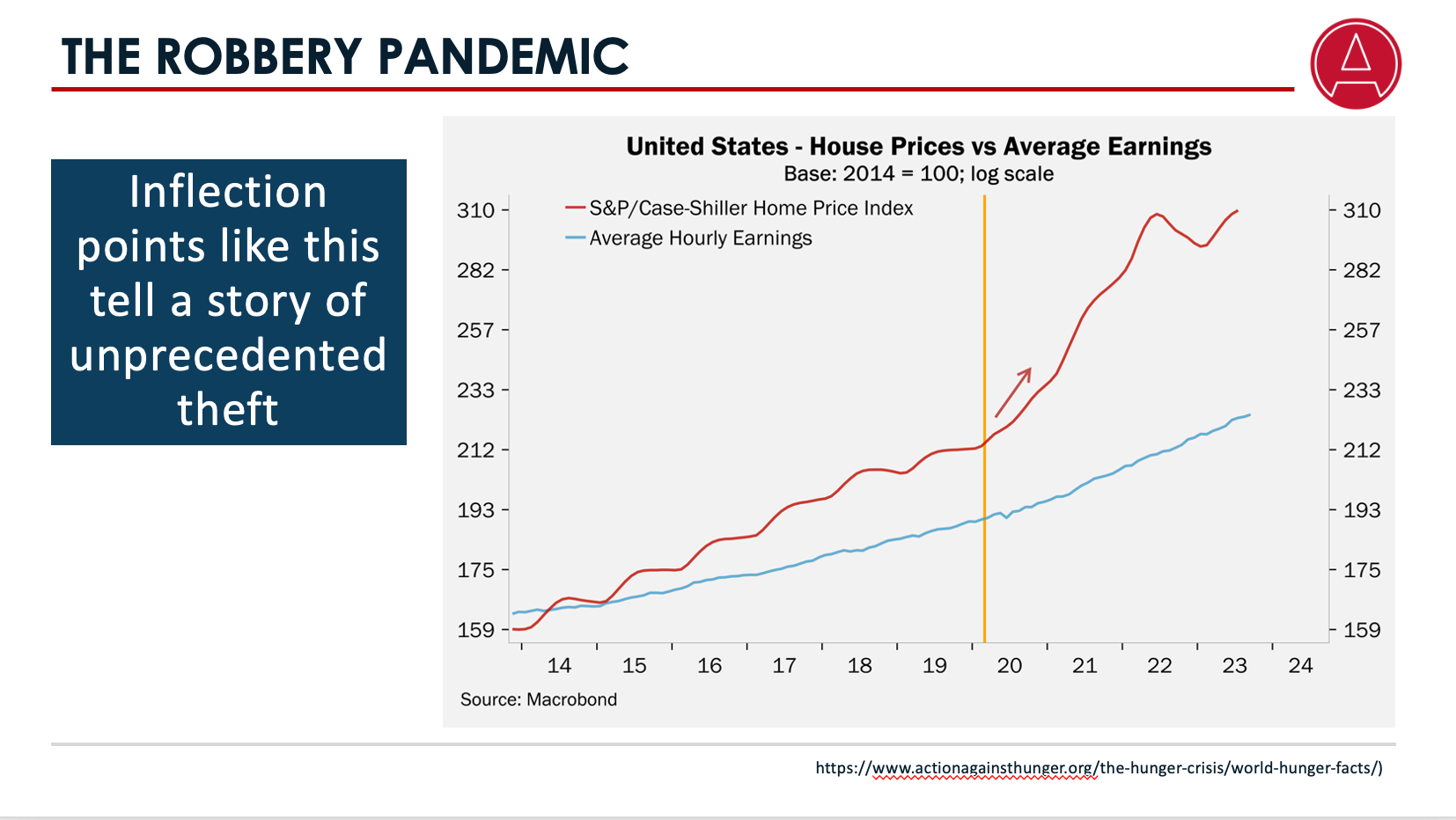
Numbers take time to be updated, but charts like this one tell a story of the haves benefitting at the expense of the have-nots.
This is precisely the kind of outcome that PANDA had warned of in our first paper, which stirred up so much breast-beating rage and anxiety amid people swept up by the false narrative of the Covid phenomenon.

If you’re not convinced that such people were engaged in acts of immense folly, we have an interesting tidbit for you. Let’s for a moment suspend judgment on the application of SIR models.

What happens when you deploy such models reflecting one of the clearest and earliest available empirical results, namely that Covid exhibited intense age-graduated mortality, with deaths among even vaguely healthy under 70s being negligible? What happens if you incorporate differential mobility for the at-risk elderly?
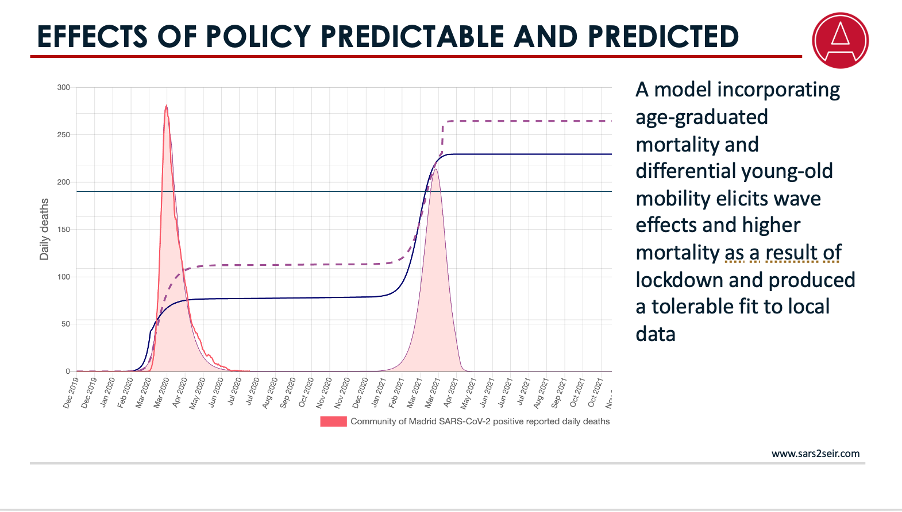
At this website we have a model you can play with showing that reducing the mobility of the non-vulnerable by locking down causes herd immunity to be attained with higher prevalence among the vulnerable. Let that sink in for a minute. What it means is that, at least in terms of the basic logic of SIR models, lockdowns can clearly be predicted to shift disease burden onto the people most likely to die, causing total deaths to increase.
OK, having argued that application of SIR models is invalid, we need to get back to reliable findings. We now have 100s of studies validating this one from PANDA’s paper in mid 2020.
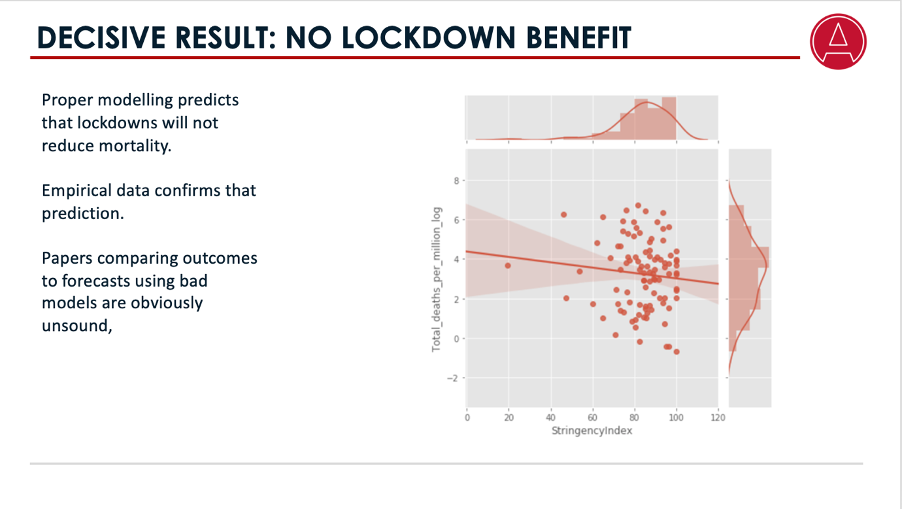
Lockdown stringency was entirely uncorrelated with official mortality data. On the x-axis we have lockdown stringency and on the y-axis, official Covid mortality. This is a paint splat.
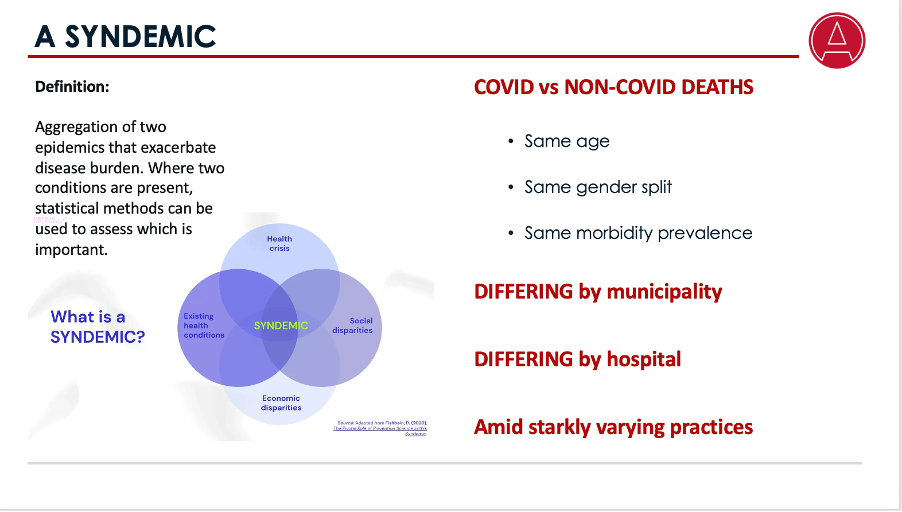
Now we return to the point mentioned earlier—that one of our first conclusions was that something else was going on other than viral spread, and that it had to do with where you were. Before exploring what that something is, let’s explore the theoretical framework. A “syndemic” is the aggregation of two epidemics that exacerbate disease burden. Where two conditions are present, statistical methods can be used to assess which is important. One of those methods is Bayesian analysis. You look at which of the two factors results in differentiation of the objective population. And we get some very clear, and, for some people, startling findings. When the presence of a Covid flag is assessed we find that the characteristics of Covid deaths are identical to the characteristics of non-Covid deaths along multiple dimensions—age, gender, income and co-morbidity prevalence. This strongly suggests that Covid is not a causative agent.
But if you flag people for where they were when they died, the proportion of death varies spectacularly by that flag. Deaths attributed to Covid emerge to be heavily determined by political boundaries at multiple levels of granularity. The combination of these two results strongly suggests that variation in clinical or public health practices is a major culprit. A second, syndemic phenomenon was operating in the background, beyond the reach of media attention.
If this strikes you as difficult to digest, I invite you to indulge in a thought experiment. Imagine that one day, when no particular virus or bacterium or fungus was in circulation, you woke up to find your local hospital administrator announcing on television that certain changes would be made to his hospitals’ policies. Henceforth patients with flu-like symptoms would be isolated; they would receive massively reduced attendance by healthcare workers; they would no longer receive antibiotics to suppress secondary infections; crucial patient advocacy provided by the hospital visitation system would be terminated; the hospitals would administer Remdesivir, a drug of no demonstrated efficacy and associated with multiple organ failure; the patients would be put on ventilators, even when they had no kinetic difficulty breathing, partly to prevent suspected aerosolization of viral particles that might endanger hospital staff, and even though the ventilator mortality rate was running at well above 90%. If that announcement happened unde1r normal circumstances there would be a public outcry, because it would be abundantly clear that such changes would result in countless deaths. And there is your syndemic, because that is exactly what transpired under Covid. Such practices were taken up more enthusiastically in certain hospitals and districts than in others, explaining the stark geospatial differentiation of deaths.
In terms of this hypothesis, known as the healthcare fragility hypothesis, which has a rapidly increasing number of adherents due to the multiple data points supporting it, the Covid phenomenon is best viewed as a mass casualty event, rather than as a viral pandemic.

So far the contents of this presentation have been quite bland and uncontroversial. Before I turn to the hot button of the injections, let me loosen you up with some salient facts. The following statements are all true, and presented in temporal order:
1. Governments signed draconian contracts committing them to acquiring billions of injection doses prior to the dissemination of any evidence regarding their safety and efficacy.
2. The results of randomised trials run by the manufacturers of those injections were released. These trials were underpowered, were not double-blinded, and groups vulnerable to severe Covid outcomes were under-represented.
3. Analysts of those trials demonstrated, using the trial data, that the intervention arm of the study exhibited worse all-cause experience under all relevant clinical outcomes than the placebo arm. The intervention arm suffered higher all-cause deaths, higher all-cause hospitalization rates, …

more serious adverse events, …
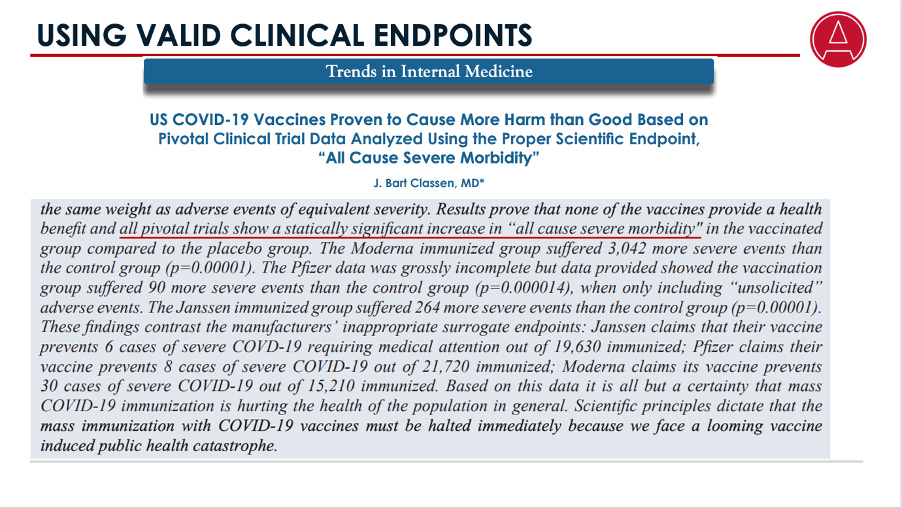
… higher all-cause severe morbidity …
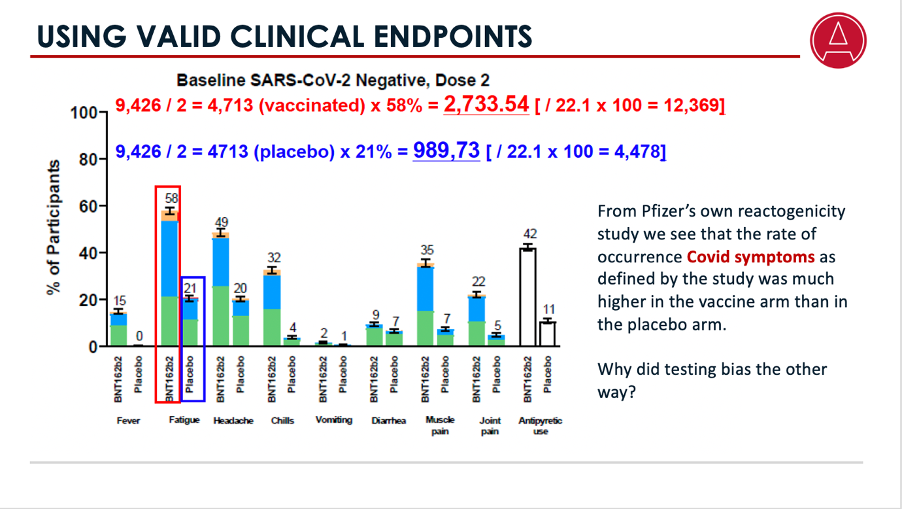
… and higher occurrence of Covid symptoms as defined by the study.
4. Media claims of 95% efficacy were made premised on one non-clinical finding from the study—that of higher incidence of Covid symptoms in conjunction with a positive PCR test.
5. Analysts found that the propensity to apply PCR tests to those with Covid symptoms in the placebo arm was multiples higher than the similar propensity for the intervention arm, suggesting profound crossing of the blind and invalidating that sole non-clinical result.

6. A legal case was brought by a whistle-blower citing multiple serious irregularities at labs to whom administration of the trial had been outsourced. Pfizer’s defence in that case was not that no fraud had been committed, but essentially that it had served up the fraud demanded of it by the US government. The Fifth Circuit judge did not accept this defence, but ruled that while those irregularities were problematic, they were not evidence of commercial fraud, because the contracts had been signed prior to commission of the scientific fraud, and that the fact that the FDA hadn’t done its job, in that it “authorized” rather than “approved” the vaccines, left the matter out of his hands.
7. Then, perhaps most significantly of all, Pfizer performed a “bait-and-switch”. It distributed to the world a product different from the one it had fraudulently tested in crucial regards.
8. Pfizer and the FDA went to court in an attempt to prevent the exchange of data between them from becoming public for 75 years.
It’s important to note that Pfizer never responded to the allegations regarding the clinical findings of the trials, even though a central and early voice and primary author in the fracas was a respected, long-serving editor of the British Medical Journal.
This is stunning, because the implication is that anyone who has ever recommended that anybody be vaccinated with their product is wittingly or unwittingly arguing that even though the product is expected to make you more likely to become sick, to experience severe illness, to be hospitalized and to die, you should take it so we can have fewer positive PCRs. And that is, quite clearly, a ridiculous proposition.
With these facts in mind I invite you to put aside whatever the man on the TV has told you about the injections and consider some data.
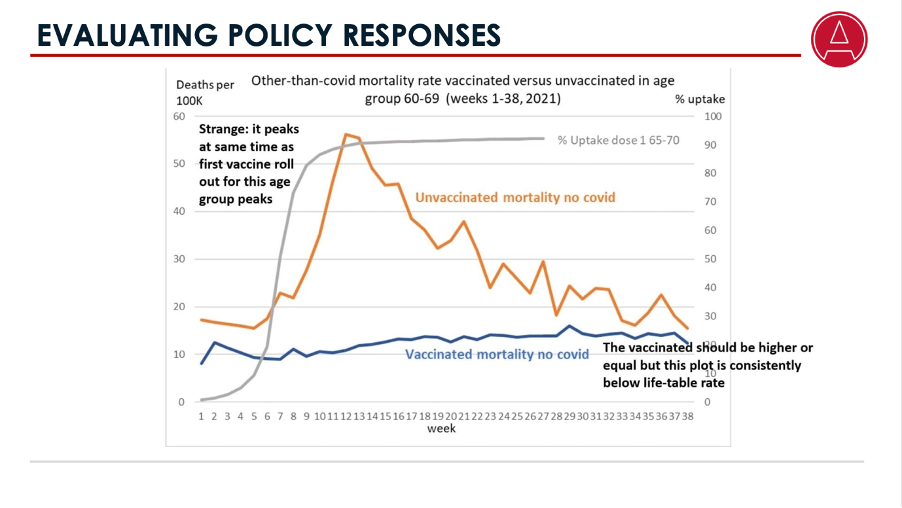
Much of the evidence presented in favour of the injections is classed as observational, as distinct from arising from a randomised control trial. This is sketchy at best, because it is very difficult to design observational studies to eliminate confounding factors. The single most relied-upon analysis regarding the injections is arguably that emanating from the UK’s ONS, or Office for National Statistics. Based on aggregate data, it claimed that the vaccines had high efficacy deeply at odds with the all-cause results from the Pfizer trial.
After much foot-dragging, the underlying data was released, and researchers immediately demonstrated significant problems visible in the underlying data. For example, consider this analysis of age-classified non-Covid mortality from that data. The grey line superimposes injection uptake on this rather strange non-Covid mortality line for the unvaccinated, depicted in orange. And once you’ve seen that, all credibility you may have attributed to that study should evaporate. Absent a coherent explanation for how the act of injecting a grandpa over here causes an uninjected grandpa over there to drop dead, all judgments based on that data need to be suspended.
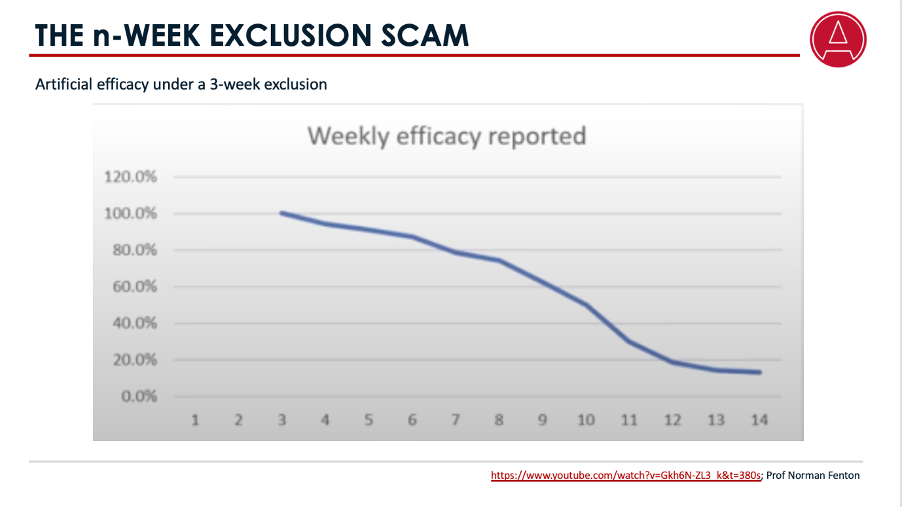
This is a distinct issue from the canard of categorizing people as unvaccinated for the first however many weeks after vaccination. Researchers have demonstrated that this approach will, mathematically, artificially induce almost arbitrarily high efficacy even if an observational study was unwittingly comparing one placebo with another.
A model outcome using a 0-week exclusion is obvious. The efficacy read when comparing a placebo with a placebo will clearly be 0.
Moving to a two-week exclusion window, the efficacy measured after 6 weeks suddenly shoots up to 60%.

And moving to a three-week window, which is what the ONS uses, the efficacy climbs further to around 80%. And all of this is, of course, entirely artificial. And of course what happens in many such observational studies is that the study is terminated after 6 weeks, because the results were so good!
Yet this scam is an almost uniform feature of investigations into injection consequences. Pointing out that Groote Schuur Hospital was deploying it elicited what was perhaps the greatest and most co-ordinated media smear campaign I faced since I started speaking out against the madness, all of it based on complete fabrications.
As a rule of thumb, categorical studies, relying on accurate placement and control for all material confounding variables are scarce as hens’ teeth. What to do? For our money, the most reliable form of investigation plausible is to conduct temporal correlation assessments of all-cause mortality. Here’s one:
Data from the Netherlands is uniquely valuable because that country conducted its vaccine roll-out in a strictly age-based fashion. Each and every age group produces a chart like this. The correlation between the injections and the age-group mortality is statistically significant and the researcher, the vaccinologist Dr Theo Schetters, infers a crude vaccine Dose Fatality Rate of about 2,000 per million doses, higher even than the purported fatality rate of SARS-CoV-2.

Similarly, this recent and methodologically sophisticated study deploys a temporal regime-change test to assess data from neo-tropical countries, where mortality exhibits weak seasonality. It estimates a global crude vaccine Dose Fatality Rate of 1,260 per million doses. Notably, South Africa produces the worst estimate, so perhaps we should be grateful that the vast majority of our population declined the opportunity to be vaccinated, despite attempts to coerce them that were in clear violation of multiple codes of public health and human rights.

An important note with regards to both these investigations is that the vDFR exhibited strong age-graduation, a feature which ought to be explored for the same reasons outlined earlier with respect to Covid mortality in the discussion of syndemicity.
Now, it takes a while for research like this to come to light, not least of all because we are often forced to undertake the costly step of deploying freedom of information requests to obtain data that should never have been out of the public domain in the first place. But there were early warning systems in place, and they were sounding an unprecedented alarm.

VAERS, a signalling system for adverse events in the US, which the FDA is very proud of, not to mention legally obliged to maintain in good working order, and in respect of which it is a felony to input false records, was sending a signal orders of magnitude higher than any ever seen. People spectacularly committed to lying tried to make out that the records were input by antivaxx members of the general public, a claim that does not stand up even to modest scrutiny. Even worse is the claim that vaccine injuries are really Long Covid, a condition for which no sound clinical definition exists, and which has failed every sound statistical test to verify its existence. They claim this even to explain the massively elevated rates of cancer and heart deaths being witnessed the world over. And the worst thing is that they know that we know that they’re lying.
When it comes to claims regarding the impact of the vaccines on Covid transmission, the warning signs came far earlier. By decades, in fact. Research into the question of whether serum antibodies are sufficient to elicit the mucosal immune response necessary to prevent infection and transmission had been consistent and clear. There was no sign of such an effect. And when it came to the Covid injections, among the earliest findings, admitted to even by the sainted Anthony Fauci himself, was that there was no difference in viral titres between vaccinated and unvaccinated people.
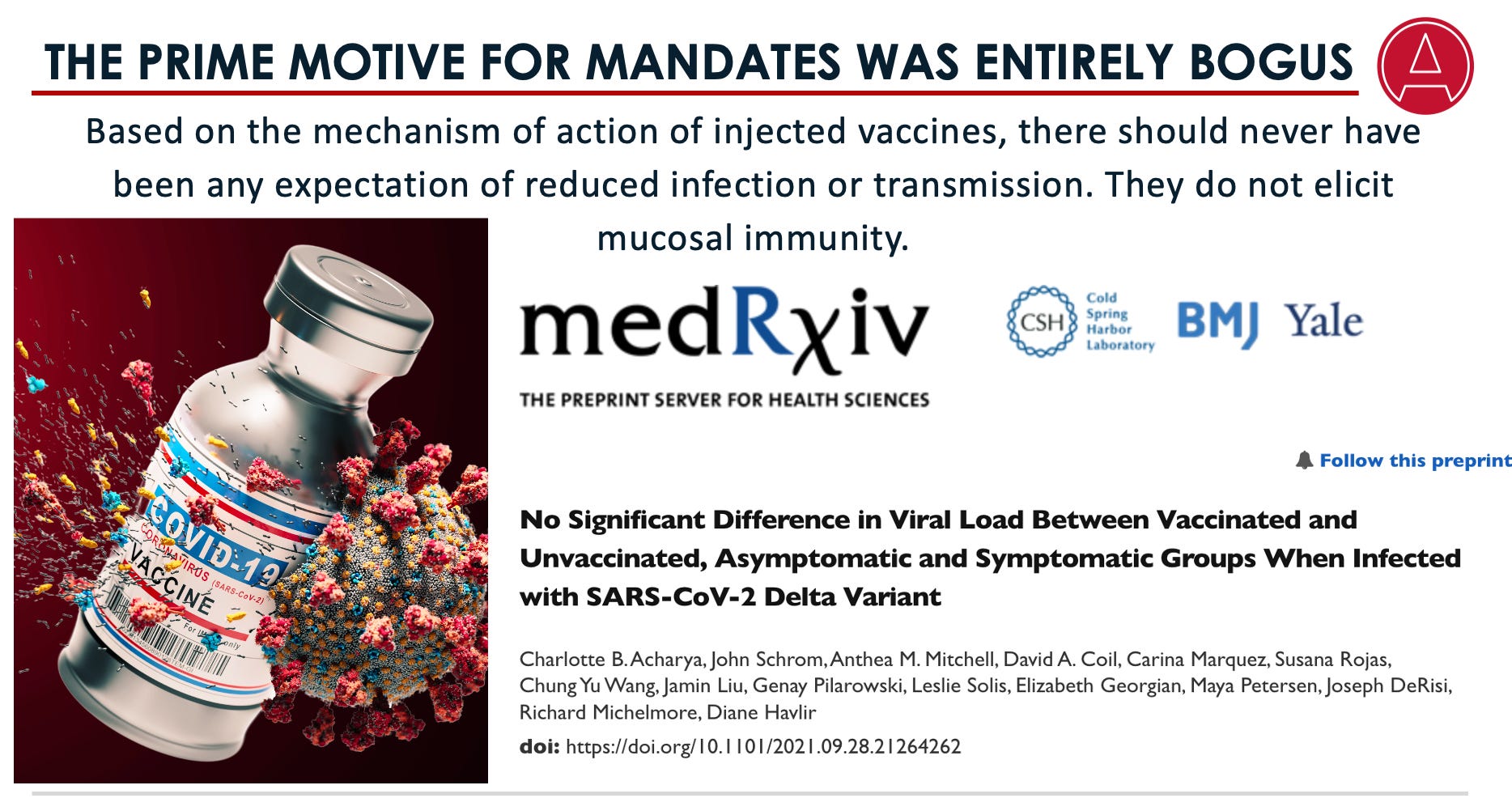
Yet despite the non-existence of any plausible mechanism for transmission suppression, and in the face of abundant evidence that there wasn’t any, the lie of transmission reduction poured forth from the mouths of not just Fauci, but diverse characters such as Joe Biden, Rachel Maddow, Albert Bourla, the CEO of Pfizer and Bill Gates. Given that transmission reduction was the prime and virtually the sole motive behind vaccine mandates, this was a particularly disgusting turn of events.
A somewhat depressing reality to acknowledge is the sheer lack of commerciality entailed in accepting the received narrative around the Covid phenomenon. By day I run a successful private equity fund. Private equity management firms suffer a very high mortality rate, principally because few people are able to sustain the degree of skepticism necessary in an environment characterised by asymmetric information. The lesson every would-be private equity transactor has to learn in order to avoid obliteration is that claims made by people whose financial well-being entails making those claims are to be assigned very low credibility.
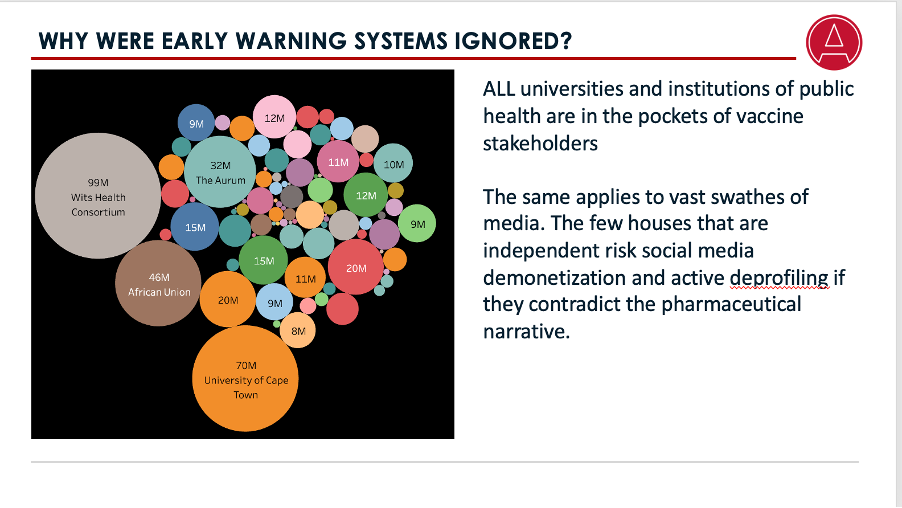
The uncomfortable reality is that all of our media, universities, institutions of public health and relevant regulators are deeply in the pockets of pharmaceutical stakeholders. Officers of these institutions are able to speak out only if they are willing to see their careers destroyed. Therefore, almost anything they do say about the Covid narrative must logically be ignored. Dictums such as “follow the science”, and appeals to the authority of such creatures should ring entirely hollow.
In a similar vein, common sense dictates that, under such conditions, it is wise to look at who is trying to censor or cancel whom. Throughout history, censorship has never been the objective of the good guys. I’ve been reminded so many times during this saga of Alexander Solzhenitsyn’s great work, The Gulag Archipelago. His notions of the “banality of evil” and how the “line between good and evil runs through every human heart” have never rung truer for me. It is the rule, not the exception, that people who commit evil acts are sincerely convinced of their own good intentions. And an episode of evil surpassing any event in world history has befallen us these past few years and continues to befall us.
What do I mean by “continues to befall us”? As we speak South Africa and many other nations, are set to sign up to a WHO accord and a subsidiary set of International Health Regulations that make the outrages of Covid pale into insignificance. In terms of these, countries agree, whenever a public health emergency has been declared, to regard all the WHO’s health recommendations as compulsory, including mass, mandated vaccination, mandated medical examinations, border closures, incarceration or quarantine of unvaccinated and mandatory censorship. In short, whenever a health emergency is declared, the sovereignty of any nation would be suspended for as long as the WHO demands it to be. No condition other than the declaration of a threat, regardless of whether there is any demonstrated harm, is imposed, and the declaration can be made at the sole behest of the director general, with no obligation upon him to follow any sort of democratic or procedural process.
Now, agreeing to do this may well be contrary to our constitution, but what the Bretton-Woods organisations clearly signalled during the Covid episode is that non-compliance with WHO diktats results in exclusion from the global financing system, and only a handful of nations are sufficiently autarchic to survive that. The accord also expands the scope of the perverse OneHealth system, a creepy philosophy that extends the definition of health outcomes to include all sorts of non-human priorities. If you haven’t heard of that before, best you read up on it. Both documents set up a requirement for intensive and continuous surveillance for viruses and their so-called variants.
Now, they will definitely find some these, as they exist in nature all the time. And next time, they won’t even need to fabricate a bogus story about a pangolin and a bat in a bar. This can then be used for locking down populations. The CEPI 100-day vax initiative will then deliver an mRNA vaccine that will be proffered as the path out of lockdown, under peril of financial isolation. Taxpayers will fund all of this nonsense, but the profits will go to industry. The surveillance set-up and the bureaucracy behind it make it inevitable that we will have recurrent threats declared and acted upon.
The funding involved is far higher than any endemic disease—the World Bank says about $31.5b a year—but a small fraction of the profits that stand to be made. All of this, despite the fact that no broadly circulating virus has produced even a miniscule fraction of the disease burden of major infectious and non-communicable diseases. It is all perfectly bananas, and unless you’re entirely brainwashed, a recipe for disaster, for everyone except the soon-to-be minted trillionaires at the top of this epic foodchain.
It should worry you that none of this has been discussed in any parliament anywhere in the world, and the mainstream media have been completely mute on any of the significant aspects of this construct.
You will appreciate why I’m going to end by saying that I hope that this period during which we have accepted the refusal of people promoting the most damaging and extreme actions the world has ever encountered to submit their ideas to the scrutiny of their peers and to engage with their critics in public forums will come to an end soon. Maybe our discussions together now can signal the beginning of the end of that blind acceptance. A sign of this would be some injection-promoter accepting our long-standing invitation to submit their sanitized date and methodologies to us for review.
And above all, as the fog of the Covid hysteria lifts, it is my hope that more members of this profession will recover the common sense and commerciality that should be their pride and joy, and see the evil for what it has been; that they will recover their courage, and take a firm stand alongside me against the spectacular commitment to lying, and say, “no more of this abject nonsense”.
Thank you.
Addendum
This section addresses remarks made by audience members during the session and afterwards.
The valid point was made that the VAERS data would be better represented on a dose-standardized basis. I made the point that, while this was correct, the finding would be the same. Here’s a standardized chart (discussed by the analyst here) that supports my assertion:

Two actuaries have expressed incredulity at my claim that Sweden’s 2020 age- and gender-standardized all-cause mortality was in line with its ten-year average. It is hard to understand the incredulity, other than as the byproduct of the false media narrative, as neither actuary advanced any alternative calculation. Our method, which is easily replicated using data from Statistics Sweden here and here was as follows: We applied age- and gender-based mortality rates for past years to the then-latest demography from the same source (as at February 2021). This is not a difficult exercise to perform and I hope the actuaries concerned will do their homework and retract their criticism. This kind of remark is all the more frustrating because, regardless of whatever methodological quibble they may imagine they have, the broad result—that the modelers’ predictions were wildly wrong, and that lockdowns could not possibly have been the cause of their failure—would still stand, barring a massive cover-up exercise, which nobody has alleged there has been.